-
Title (Dublin Core)
-
Medical equipment for the bombers crews
-
Article Title and/or Image Caption (Dublin Core)
-
Title: How Flyers Are Redisigned
-
extracted text (Extract Text)
-
flight surgeons who faced down a myriad of
discouragements and stuck to their research
during the starvation years of military avia-
tion.
There is an unearthly, mechanistic, man-
from-Mars quality about this whole subject
of man's adaptation to an unnatural ele-
ment, which makes it difficult to keep in
mind that it all comes down to the aches
and pains, the homely frailties, of the indi-
vidual. But the flight surgeon never forgets
it. The flight surgeons for years have main- |
tained their research laboratory at Wright
Field, Ohio, and now have established sev-
eral new research laboratories at various
Air Force Stations. Through these funnel
all the findings of the various research or-
ganizations now working on the physiology
of flight. But as the service is administered
by the Air Surgeon, Col. David N. W. Grant,
their work all comes down to the individual
physician who lives with each air squadron,
practicing preventive medicine as a sort of
combination family doctor and athletic |
trainer, watching the pilots physically, men- |
tally, and emotionally, keeping them fit to
function in an element for which nature
never intended them.
The newest and most mysterious job of
the flight surgeons is the problem of night
vision. The coming of actual war in 1939
changed night military aviation immedi-
ately. The blackout was something new
to mankind. Pilots had to learn to land
without floodlights, only a few faint clews.
They had to learn to distinguish the enemy
as only a dim silhouette in the dark sky.
Their glareless instrument board, worked
out with infinite care by the flight surgeons |
and engineers, had to be darkened along
with everything else.
It soon developed that pilots with perfect
day vision showed wide variations in ability |
to see at night. Strenuous efforts still are |
being made to perfect simple, speedy tests |
to pick the best night fighters.
The photochemistry of night vision is still |
mysterious, but it is thought to be inti-
mately connected with vitamin A in the diet.
A deficiency of vitamin A causes xeropthal-
mia, an eye inflammation commonly asso-
ciated with night blindness; but the Air
Forces are interested in something much |
less obvious than that.
In the retina of the eye is a pigment |
known as visual purple, very sensitive to
dim light, formed by a combination of vita-
min A with certain proteins. Light bleaches
out the visual purple in the eye. Prevailing
theory is that adaptation to darkness de-
pends on the amount of visual purple stored
up in the eye, and that glare blinds us by
bleaching it out. Blindness follows glare
until the pigment is restored. Whether or
not this is the final solution, the flight
surgeons heavily load the diet of
pilots with butter, eggs, carrots, and
spinach to supply large quantities of
vitamin A. The flyers grumble good-
humoredly about “duty food” and put away
large platefuls of salad greens.
The structure of the eye also is important
in night vision, especially the placing of the
rods and cones, sensory bodies in the ret-
ina. The human retina, unlike that of lower
animals, has at its center a yellow spot
called the macula lutea, made up almost
entirely of cones. This macula gives us
acuity of vision, enables us to read; but it
ia no good for night vision. The periphery of
the retina is amply supplied with rods,
sensitive to light and movement, which pro-
vide the warning mechanism of the eye. It
is here the visual purple is found.
While looking straight ahead, hold your
hand at the side of the head, waggling the
fingers. Then bring it forward. You will
be conscious of motion and a light image
long before the fingers come into the field
of the macula, which focuses them sharply.
From these facts of anatomy the sur-
geons have been able to teach the pilots a
trick for seeing in the dark, a device
used by the astronomers of ancient
Egypt for hunting dim stars with the
naked eye. Often the corner of the eye
will pick up a dim light at night, but
that light will disappear if stared at
directly. The way to see faint illumina-
tion at night is to look, not straight at
it, but about seven degrees away from it.
Night vision has been found also to
have a close relationship to oxygen sup-
ply. The daytime flyer has no. special
need of artificial oxygen supply below
10,000 feet, but the night fiyer must
use it from the ground up. Night vision
starts failing at 4,000 feet without
oxygen and at 10,000 has fallen off
decidedly. The man who has been using
oxygen, if glared by searchlights at
10,000 feet, will get back his vision in
three or four minutes. Without oxygen
it will take him more than ten times as
long.
Now that American planes have at-
tained a top diving speed of over 600
miles an hour, and the structural
strength to pull out of such a dive, it is
a commonplace that our ships are bet-
ter than the men who fly them. Speed
itself is no hazard, so long as the cock-
pit is inclosed; all of us are moving 12.4
miles per second with the surface of the
earth, But the instant high velocity
varies from a straight line, in a zoom
upwards or a horizontal turn, the ordi-
nary pull of gravity is multiplied by
centrifugal force—by five, six, even ten
times or more. In a seven-G turn a pilot's
weight is multiplied seven times. His blood
weighs as much as molten iron.
Continue this force more than an instant,
and the pilot sees mist before his eyes, then
a graying, then a “blackout” leading
toward complete unconsciousness, as blood
is drained irresistibly away from the brain.
A healthy young pilot can usually stand
from 5 1/2to six G's for three seconds with-
out blacking out, but he probably pushes
himself and his piane harder than that. The
pursuit pilot takes the blackout for granted,
‘as merely a part of the day's work.
The fight surgeon has never been will-
ing to accept this view. He is supported by
recent British studies with a motion-picture
camera fixed on a pursuit pilot in action.
In relation to time and instrumental re-
cordings of the force applied, the films
graphically show the face muscles sagging
under multiplied weight, the blank expres-
sion of the eyes, the lapse into the uncon-
scious. Blackouts last longer than pilots
suspect. Often they pass out completely
without realizing it.” Such things mean loss
of combat efficiency, and the blank moment
may be the instant when the fight is lost. |
A slight change in posture may greatly
increase the pilot's resistance. Merely rais-
ing the feet six inches has increased resist-
ance 1 1/2 G's. Prewar studies with a cen-
trifuge in the Air Research Institute in Ger-
many showed that a person lying on his
back could stand a pull of 15 G's for thirty
seconds—though beyond ten G's he found it
almost impossible to lift his chest against
the force for breathing. Standing is the
worst position; a sudden force of 4 1/2 ; G's
has been known to break a man’s leg. Pilots
carrying infantry and parachute troops on
their feet have to watch out for this.
Anything which shortens the blood col-
umn in relation to the pull of centrifugal
force increases the resistance to it. One rea-
son for this is that the heart provides a
limited amount of blood pressure, and the
head to function properly needs pressure
equivalent to a column of water 50 centi-
meters high.
The man with 160-cm. blood pressure at
the heart has 110 cm. available to lift his
blood to the head. At one G, normal grav-
ity, he needs 30 cm. to lift the blood; at
two G's he needs 60 cm. Theoretically he
will reach his limit at about 3 2/3 G's.
An important factor is the draining down-
ward of the heavy blood out of the head,
into the lower parts of the body, and its
difficulty in rising back to the heart. If the
force continues, the blood vessels in the
abdomen expand and pool large quantities
of blood, reducing the supply back to the
heart and thereby cutting pressure. A
circulatory collapse may result from this,
causing long unconsciousness, but unless
the flyer is in bad physical condition it does
not happen in the few seconds of an air-
plane turn.
If the fiyer leans forward, lowering his
head ten cm., or four inches, he needs only
20 cm. of pressure to lift blood to his
brain. With 110 cm. available he can get up
to 5.5 G's in this position, before reaching
his limit. If he is one of those individuals
whose blood pressure increases under ex-
citement, a total pressure of 210 cm. will
give him a resistance of eight G's.
Tall, slender men with long blood columns
don't make good pursuit pilots. They black
out easily and tend toward low blood pres-
sure. Chunky men tend to run a high blood
pressure when excited. Theoretically, the
ideal pilot to resist multiple G's would be a
squat old man with high blood pressure and
hardening of the arteries—blood vessels so
rigid they would not expand to pool blood
in the abdomen. That is, he might be good
until his heart or a blood vessel failed.
All this has dealt with downward forces.
If the wing load of a plane is reversed, as in
an outside loop, the effect is different. Blood
rushes to the head at high pressure. At only
three G's the pilot is likely to “red out” and
only a slight increase may bring uncon-
sciousness and brain hemorrhage. Pilots
flying upside down have to be very careful.
The most practical flying position for
dive bombers and pursuit pilots continues
to be seated, with feet on high rudder pedals
and shoulders bent far forward. Jackknifed
in this fashion, the pilot naturally constricts
his abdominal muscles, holding in the blood
vessels, and this effect may be increased
by tightening a belt across the abdomen.
Once bent forward, the head and shoulders
are automatically carried farther down by
centrifugal force.
Men have dreamed of fast pursuit ships
flown like a sled, bellywhopper. But a pilot
on his stomach cannot hold his head up
without special support, and cannot breathe
with all that weight on his chest. Seats
have been devised which tilt back, but
the posture is better adapted for getting
a shave than for mortal combat. Lying on
the side might work.
Developments of this sort will require
changes of cockpit design, controls, and
pilot training. Intensive secret efforts
toward such ends are being pursued both
in this country and in Germany. We have
an experimental centrifuge said to be bet-
ter than that of the Germans; whirling on a
24-foot diameter, it can apply its high
forces almost instantaneously. We are not
lagging. When you hear of American planes
in Libya turning inside the Messerschmitts,
that means that the pilots are taking
stronger forces than the Nazis. And, de-
spite the flight surgeons, they doubtless
still are blacking out. Those young devils
drive themselves and thelr planes to the
limit. What the medical men have done
is to increase the effective—or usuable—
speed and maneuverability of the airplane.
The frontier of altitude is being con-
quered rapidly. Two years ago a flight to
30,000 feet was a rarity. Today flights to
35,000 and better are made regularly, by
test pilots at least. As for the flight sur-
geons, thelr research men work daily in
low-pressure-chamber equivalents of 40,000
feet and more. For some time we have been
saying that airplanes could fly higher than
their pilots. Today it is beginning to be
doubtful whether this is longer true.
Adrplanes have mechanical difficulties at
high altitudes which are not all solved by
the supercharger. Supercharged air needs
to be cooled for the engine after compres-
sion, and while bombers easily carry the
additional weight of the cooler, it is difficult
for pursuit ships. In some ships magnetos
and crankcases have had to be super-
charged. Fuel has started to boil away at
low pressure. Lubrication has failed in the
cold. We don't ordinarily hear about the
high-altitude attempts which don't suc-
ceed.
Medical problems of high altitude have
also been largely mechanical. Operations
at 40,000 feet are made possible by an
oxygen mask. At this low pressure men
are coming close to the ceiling of existence,
without either pressurized cabins or pres-
surized suits. Up to 40,000 feet the oxygen
saturation of the blood can be Kept up close
to normal, but after this it falls rapidly and
the absolute ceiling is in the neighborhood
of 45,000, for selected personnel only.
Man adapts himself to living high in the
mountains by producing more red cor-
puscles in his blood, but daily flights of
several hours are not enough to bring this
about. He ls dependent on the laws of
Physics and the behavior of gases at vari
ous pressures, inside and outside the lungs.
Even breathing pure oxygen, he comes to
the point. where he can't get enough to
‘maintain himself, and this development of
anoxia, or oxygen lack, proceeds much
more rapidly in the last 16,000 feet than one
‘might suppose.
To understand this, let us start theo-
retically at 51000 feet and work down. At
this altitude the atmospheric pressure is
equal to u column of mercury 87 millimeters
high. Now at all levels, from the ground
up, the space Inside the lungs n saturated
wiih water vapor, with a constant pressure
of 47 millimeters. Body metabollam_pro-
duces carbon dioxide at a rate which keeps
its pressure in the lungs practically con-
stant at 40 mm, Together the water vapor
and CO, make up 87 mm. of pressure, and
there 1a no room for any oxygen whatever
to got into the lungs.
Now let us come down to 40,000 feet.
Here the atmospheric pressure Is about 141
mm, enough to allow a lung pressure of
50 mim. of oxygen. That is the critical level,
enough to keep the blood 80 to 85 percent.
saturated with oxygen, Below this pres-
sure, saturation rapidly falla to a danger.
ous level.
Coming down to 33,000 foot, we find the
atmospheric pressure is enough to allow a
pressure of 100 mm. of oxygen in the
lungs (assuming the oxygen mask is deliv-
ering pure oxygen). This 106 mum. a the
normal amount of oxygen in the lungs at
sea level.
Without an oxygen mask, a man reaches
the critical pressure at about 12,000 feet and
the ceiling around 25,000, for the atmos-
phere is only 21 percent oxygen.
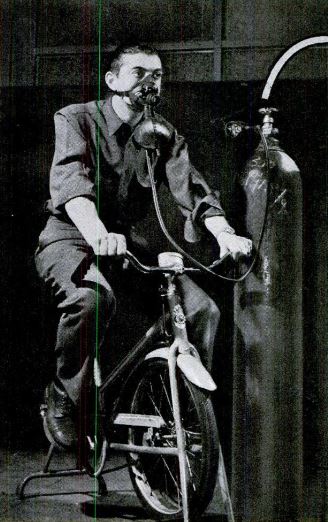
High-flying pursuit pilots don't have to
use much physical energy, but bomber
crews have to move around, and that work
uses up oxygen. In the low-pressure cham-
bers today at 40,000 feet they are studying
this use of oxygen in detail. The subject,
wearing his oxygen mask, lifts weights to
use up the oxygen in his blood. Attached
to his ear is a device called the oximeter,
which filters light through his ear and
‘measures the changing color of the blood
with a photoelectric cell.
Slight efforts make a remarkable differ-
ence. Shivering, for instance, is the body's
involuntary way of getting warm. This
“work” increases the basal metabolism
rate by four or five times, and uses up
that much more oxygen.
The cold, 55 or more below zero in the
substratosphere, is thus intimately con-
nected with the use of oxygen as well as
comfort, for heat comes from oxidation.
If a fiyer gets cold at 15,000 feet, a few
breaths of pure oxygen will warm him up.
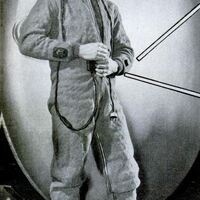
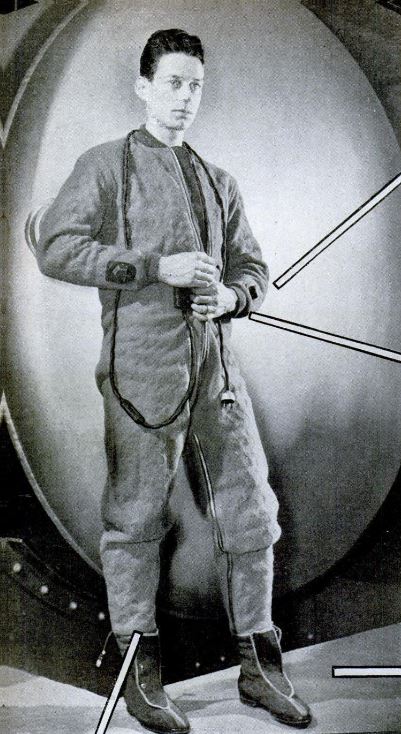
To avoid great bulkiness of clothes, elec-
trically heated suits have been developed.
Some of these merely heat the hands and
feet, but as to this care must be taken. If
the extremities are warmed too much, that
stimulates the
skin of the rest of the body to lose heat
much more rapidly.
With pressurized suits or pressurized
cabins, it would not be necessary to skate
on such a thin edge of oxygen. So far,
pressure suits are too clumsy to be very
useful, and for military uses pressure cab-
ins are dangerous. Small bullet holes can
be easily patched, but a broken window or a
hole from an explosive shell would be dis-
astrous—at 51,000 feet, for instance. Pres-
sure cabins are commercially useful for
comfort at much lower altitudes, and the
Air Corps has experimented with them suc-
cessfully. But in combat at high altitudes
the men inside will still have to use masks
and have emergency oxygen flasks for para-
chute jumping.
It waa only in 1939 that the oxygen mask
came into use in our Air Corps. Before that
the fiyer took oxygen from a pipe stem held
between his teeth, and it fed him a constant
flow from a compression tank. The mask in
common use today, developed by Drs. Booth-
by, Lovelace, and Bulbulian of the Mayo
Clinic, 1s a far cry from that; and even
this BLB mask is now obsolete for combat.
The BLE mask fits tightly over the nose
and mouth. Oxygen flows at constant rate
(fixed manually according to need) Into a
rubber bag, from which the flyer sucks his
breath. When he exhales, the first 150 cc.
of the exhalation is pure oxygen which
never got to the lungs, and it goes back
economically into the rebreather bag. When
the bag is full, the rest of the exhalation
goes out through a sponge-rubber disk, in
a turret In front of the mouth. Moisture
from the breath collects in the sponge rub-
ber, and in an unheated cabin it is likely
to freeze up tight. The mask turret also
gets in the way of the bombardier's sight.
One mask has eliminated the turret and
it has its breathing apparatus down Inside
the fiyer's clothing, where body heat keeps
it from freezing. This mask is equipped
With a valve which automatically feeds the
right quantity of gas from tho tank, as the
flyer inhales. Development of such vaives has
been one of the most difficult designing jobsin
the development of oxygen masks. No mat-
ter how dry the oxygen was, they were
likely to freeze up. This was especially true
formerly when oxygen was carried in tanks
at a pressure of 1,800 pounds to the square
tnch. Tn addition to the cold of altitude, the
expansion of this gas through the valve
had an effect of refrigeration, and lowered
the temperature by several degrees more.
Only a certain number of men in the Air
Forces are able to work at the highest alti-
tude. Others are afflicted above 30,000 feet
by aeroembolism, known to sandhogs and
divers as the “bends.” At extremely low
pressure, atmospheric nitrogen dissolved in
the blood is discharged as bubbles, like the
gas in an opened soda-water bottle. This
causes itching, rash on the skin, and some-
times excruciating pains. By breathing pure
oxygen and exercising before leaving the
ground, it has been found possible to wash
most of the nitrogen out of the blood. But
with some men this doesn’t work.
One of the hardest jobs of the flight sur-
geons is to persuade flyers to accept their
findings, especially as to the need of oxygen
between 10,000 and 15000 feet. The first
effect of anoxia, oxygen lack, is a feeling
of exhilaration and well-being—much like
the notion of a man, after a half dozen
cocktails, that another little drink wouldn't
do him any harm.
18 8 Navy (OW-presgure Chan ver, at ou,
000 feet, a flyer once impatiently removed
his mask. Horrified doctors hurried to in-
crease the pressure, meanwhile held a stop-
watch on him. He collapsed in 35 seconds.
Another Navy flyer learned his lesson in a
strange way.” Flying above 20,000 feet one
day without oxygen, he noticed that his in-
strument board lacked a bank indicator.
Diving to lower altitude, he looked at his
instrument board and found the bank in-
dicator back in its proper place.
Pilots flying all day at 15,000 feet with
oxygen are warmer and suffer less fatigue
than if they fly at 8,000 feet without oxygen.
All pilots are supposed to use oxygen above
10,000 feet, but the pilot of a single-seater
is pretty much his own master when he
gets in the air. He needs to be convinced.
The flight surgeons are now installing
more than forty altitude chambers in vari-
ous parts of the country for indoctrination
of members of combat crews. A machine
gunner is put in the chamber with one of
those nickel-in-the-slot machines which
shoot light beams at moving airplane tar-
gets. He starts out making a fine score,
and as pressure is decreased he fires away
with increasing confidence, but with rapidly
deteriorating marksmanship until he can’t
hit the target at all. Then he is given oxy-
gen and immediately the shooting improves.
The pilot, watching the procedure, learns
his lesson as well as the gunner. —HICKMAN
POWELL
-
Contributor (Dublin Core)
-
Hickman Powell (writer)
-
Language (Dublin Core)
-
eng
-
Date Issued (Dublin Core)
-
1942-05
-
pages (Bibliographic Ontology)
-
117-123, 222, 224
-
Rights (Dublin Core)
-
Public Domain (Google Digitized)
-
Archived by (Dublin Core)
-
Roberto Meneghetti
-
Marco Bortolami (editor)


 Popular Science Monthly, v. 140, n. 5, 1942
Popular Science Monthly, v. 140, n. 5, 1942