-
Title (Dublin Core)
-
How U.S. medical soldiers operate on the battlefield
-
Article Title and/or Image Caption (Dublin Core)
-
Title: How medical soldiers meet the Blitzkrieg
-
extracted text (Extract Text)
-
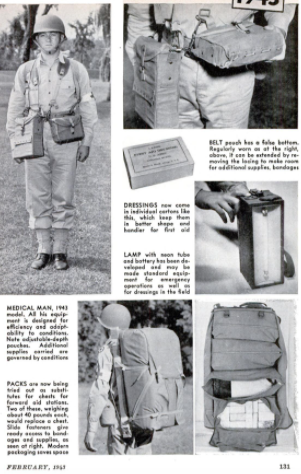
MECHANIZED warfare has brought
new problems to the Army's Med-
ical Department. Even on a rela-
tively static battle front, like those of the
first World War, the task of aiding and
bringing back the wounded is a gigantic
one. In fluid blitzkrieg fighting, with the
tide of battle rolling rapidly over miles of
countryside, the medical men must wage a
blitzkrieg of their own—in reverse.
‘Win, lose, or draw, the Medical Depart-
ment has its hands full. When things go
badly, it may find itself responsible for 25
percent of the total personnel engaged in a
given sector. When things go well, the per-
centage of wounded is likely to be less, but
the very success of the operation introduces |
new difficulties. A clearing or sorting sta-
tion for the wounded which was located six
miles behind the front at the beginning of
the attack may be 20 to 30 miles behind |
after a few hours. Yet the medical units are
bound to keep up with the movement some-
how, for time is precious. The sooner a seri- |
ously wounded man can be picked up, given |
first aid, and evacuated, the better his
chances of survival. The farther back he
goes the more comfortable he can be made
and the more adequate the treatment which
can be given him.
The illustration at left below is a sche-
matic representation of our Army’s current
arrangements for handling the wounded.
From right to left, the sketch shows the
combat area between the battle front and
the nearest railhead. Evacuation is carried
out in stages or echelons. The zone between
the battle line and the collecting station or
assembly point, normally about 1 1/2 to two
miles in depth, is called the first echelon. In
this zone all service to the wounded is ren-
dered by medical personnel attached to the
line units. The second echelon begins at the |
collecting station and extends to the clear-
ing station five to eight miles behind the
line of departure. This is a divisional zone,
in which service is rendered by the division
medical units. Still farther back, in the
third echelon, the medical units attached to
an army, which consists of several corps and
divisions, take over the casualties.
In the battle area itself, essential first aid
is given to the wounded, under whatever
cover can be found, by first-aid men at-
tached to the companies in combat. The
next step is to get the wounded back to bat- |
talion aid stations some 300 to 500 yards be-
hind the front line. These field dressing sta-
tions usually afford shelter from rifle fire,
but not from chance artillery hits. Every
effort is made to locate them so that the
wounded can be brought in by stretcher-
bearers under some sort of cover, as behind
a hill or ridge, and if at all possible be |
evacuated, when night falls, in vehicles
rather than on foot. The normal comple-
ment of the aid station is two medical offi-
cers and seven enlisted men trained in han-
dling injuries. Here efficient temporary
dressing of wounds is possible and morphine
is available,
If the battalion moves forward the station
moves with it, the patients already deposited
being left with medical attendance until
they can be brought back, by ambulances or
stretcher-bearers, to the collecting stations.
Each of the collecting stations is fed by sev-
eral battalion aid stations. Like the latter,
the collecting stations move forward with
the combat forces. The collecting stations
are essentially intermediate medical bases
where patients are examined, sorted, and
prepared for evacuation to the clearing sta-
tions. Between the collecting and clearing
stations an ambulance shuttle service is
maintained, During the night the ambu-
lances may be able to go all the way up to
the battalion aid stations. When this is
feasible the wounded are far better off, for
it is in the first echelon that the worst bot-
tlenecks occur.
The division clearing station is usually
out of medium artillery range, and on a
good route to both
the front and the rear. Here a more careful
sorting of casualties takes place. Some may be
found fit for duty and returned to the front.
Others, who require operative treatment, are
taken care of by a mobile surgical unit at-
tached to the clearing station. Thence the seri-
ous cases are sent back to the evacuation hos-
pital, which normally is located at a railhead or
airport where hospital trains or planes are
available to take them out of the combat zone
as soon as they are fit for the journey. Less
serious injuries are treated at a convalescent
hospital in the same neighborhood. After dis-
charge these are sent to a replacement depot
and returned to the front.
‘The foregoing will give the reader some idea
of the transportation difficulties involved in
giving first-aid and evacuation service to the
wounded. Yet it presupposes a relatively slow-
moving tactical situation in which the disabled
man has to be carried only a few hundred yards
on a stretcher before he is laid on a table be-
fore a medical officer. Suppose, however, that
the injured soldier is in a tank operating with
an armored division. There is no room for
company aid men in tanks. Members of tank
crews are trained to take care of their own
emergency cases, using vehicular first-aid kits
carried in the tanks. The company aid men
follow the advance in motor vehicles and col-
lect casualties along a central axis of evacua-
tion. They then get their patients to the rear
from prearranged rallying points. Half-track
armored vehicles which have carried armored-
division infantry behind the tanks are often
used for this purpose. These half-tracks are
equipped with litter braces so that they may
be used as improvised ambulances.
‘Who are the men responsible for the health
of the millions of Americans already in the
Army and the millions who will soon join
them? Where do they come from and how are
they trained? Some civilians have an idea that
most of the Medical Department's personnel
consists of physicians. The fact is that out of a
total strength of 125,000 before Pearl Harbor
(current figures are restricted), only 183,000,
or a little more than 10 percent, were offi-
cers, and not all of these were physicians.
In World War I the Medical Department
numbered 400,000—an army within an army.
There is nowhere near that number of li-
censed physicians in the United States. Ob-
viously, while physicians provide the mili-
tary and scientific leadership in the Medical
Department, the bulk of the routine work
must be done by officers other than Medical
Corps physicians. This calls for a gigantic
training program.
Today, the Medical Department is operat-
ing four medical replacement training cen-
ters and nine special-service schools. Men
are assigned to the schools on the basis of
civilian occupa-
tion and aptitude as determined by classifi-
cation tests. The schools have a combined
yearly capacity of about 160,000 trainees—
35,650 basically trained medical soldiers can
be delivered to medical units or installations
every 10 weeks.
Medical transportation is a vital factor,
not only in saving the lives of sick and
wounded men, but in maintaining the mo-
rale of the whole Army. Once a unit gets
into action, good morale implies the indi-
vidual soldier's willingness to die to gain a
vital objective. But the soldier knows that
he may neither escape unscathed nor be
killed; he may be wounded. In that case
he wants to be taken out of there—fast. If
he has confidence in the Medical Depart-
ment’s ability to move him with the least
possible delay, and to give him every pos-
sible chance for life, he will be a better
fighting man.
~The ideal ambulance will go almost any-
where, provide a comfortable ride for the
patient, and go as fast as is consistent with
safety. The latest Army motor ambulances
fill these specifications adequately and are
cheap to build. The body is mounted on a
standard Army half-ton chassis with four-
wheel drive. The gross weight with a 1,500-
pound “payload” is 6,670 pounds, and the
speed is anything from 2 1/2 to 55 m.p.h. on
roads. The vehicle can go cross-country if
the terrain is not too rough. The body is of
20-gauge steel, thermally insulated, and hot
water from the engine maintains a 70-de-
gree temperature when the outside tempera-
ture is below zero. A fan changes the air in
the body once a minute. Rear doors are 58
inches wide and 47 inches high to facilitate
loading. The springs are inclosed in metal
covers to prevent rusting. An ambulance of
this type will accommodate four litter pa-
tients or seven sitting patients. The jeep
offers excellent possibilities in forward areas
as an ambulance with very slight adjust-
ments.
he Army also has a very light horse or
mule-drawn ambulance (1,130 pounds) with
an automobile body and low-pressure tires.
This will hold four men in litters or five
seated. At the other extreme there is an
ambulance of bus type, holding 12 litter pa-
tients or 20 sitting patients. This is equipped
with front-wheel drive for speeds of 21 to
70 m.p.h., and although designed for roads
can go cross-country when necessary. Plans
have also been made for converting ordinary
suszes into ambulances if resuired. It is
possible that future ambulances will be
lightly armored for protection against
small-arms fire.
Air ambulances will be used by the Army
as far as possible. The War Department re-
cently announced the formation of an Air
Evacuation Group (Medical) to evacuate
sick and wounded soldiers at top speed. It
is estimated that a trip which might take 18
hours over difficult terrain in a vehicular
ambulance can be accomplished in one hour
by plane. The planes to be used are large
transport or cargo ships which will bring in
supplies and take out the wounded. They
will be fitted with racks for standard Army
stretchers, surgical and blood-transtusion
facilities, oxygen masks, heating pads, and
other equipment for 40 patients. Each plane
will carry a flight surgeon, a nurse, and a
Medical Department enlisted man who has
been specially trained for evacuation of
wounded by air.
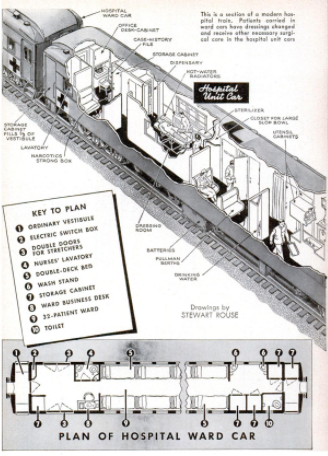
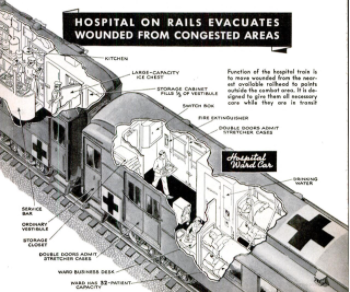
To do his best the physician or surgeon
needs adequate laboratory and operating fa-
cilities. In war the surgery and the labora-
tory have to go to the patient, not the other
way around. To design and build a rolling
surgical hospital, with its own water and
power supply and facilities for heating, ven-
tilation, sterilization, and all the other re-
quirements, is a problem which at first
seems insoluble. But the Army has de-
veloped such hospitals in both self-propelled
and semitrailer types.
The methods of treatment used in the
Army's mobile and fixed surgical hospitals
are the latest and best. The sulfa drugs
occupy a prominent place in military sur-
gery these days, and the mortality figures
leave no doubt as to their efficacy. In World
War I the mortality from perforating
wounds of the abdomen was 80 percent, The
victim had one chance in five to live, Now,
on the basis of experience in the Philippines
and at Pearl Harbor, Maj. Gen. James C.
Magee, Surgeon General of the U. S. Army,
reports that such wounds are seldom fatal,
and a large number of the men who sus-
tained serious wounds have already re-
turned to duty.
The sulfa drugs are a vital element in the
remarkable results that Army surgeons are
getting in wound therapy, but only one ele-
Last we may consider What the Medical
Department puts first—the prevention of
disease. The air lines talk about preventive
maintenance. They got the term from pre-
ventive medicine. In every war the enemy
most to be dreaded is disease. Disease kills
more men than wounds. The health of the
Army so far has been excellent. This is not
mere luck; if it were we could not rely on.
its continuance.—CARL DREHER.
-
Contributor (Dublin Core)
-
William W. Morris (Photographer)
-
Carl Dreher (Article Writer)
-
Language (Dublin Core)
-
eng
-
Date Issued (Dublin Core)
-
1943-02
-
pages (Bibliographic Ontology)
-
126-133, 228, 230
-
Rights (Dublin Core)
-
Public Domain (Google Digitized)
-
Archived by (Dublin Core)
-
Matteo Ridolfi
-
Marco Bortolami (editor)




 Popular Science Monthly, v. 142, n. 2, 1943
Popular Science Monthly, v. 142, n. 2, 1943
 Schermata 2022-02-20 alle 15.08.38.png
Schermata 2022-02-20 alle 15.08.38.png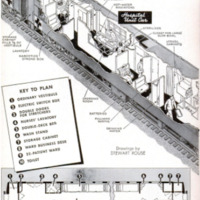 Schermata 2022-02-20 alle 15.09.11.png
Schermata 2022-02-20 alle 15.09.11.png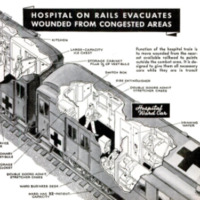 Schermata 2022-02-20 alle 15.09.21.png
Schermata 2022-02-20 alle 15.09.21.png Schermata 2022-02-20 alle 15.09.37.png
Schermata 2022-02-20 alle 15.09.37.png Schermata 2022-02-20 alle 15.09.50.png
Schermata 2022-02-20 alle 15.09.50.png Schermata 2022-02-20 alle 15.10.06.png
Schermata 2022-02-20 alle 15.10.06.png Schermata 2022-02-20 alle 15.10.45.png
Schermata 2022-02-20 alle 15.10.45.png Schermata 2022-02-20 alle 15.11.20.png
Schermata 2022-02-20 alle 15.11.20.png